|
Today I arrived at the NICU at 8:00. I immediately washed my hands and reported to rounds. Dr. Te, me, and 5 other doctors went to each baby one by one and looked over their sheets and made plans of attack for each babies recovery. About have way through rounds, each of the doctors pagers went off, meaning that a woman was having a c-section upstairs.
The resident, a med student, and myself reported to the c-section call upstairs. We had to put on shoes nets, hair nets, scrubs, and gloves before entering the OR holding room. I watched the c-section from the window and there was a lot of drama in the OR. The dad had cheated on the mom and she was angry with him and was calling him inappropriate names. There was a lot of tension and the mom was in so much pain that she started screaming. Once the baby was out the doctor brought him in the OR holding room. He was huge. The dad came in and cut the umbilical cord and the baby was cleaned off. The baby would not stop screaming. Once the doctor examined the baby and stated that it was in good health, the NICU doctors and myself left and went back to the NICU. When we got back the doctors hadn’t finished rounds so we joined back into that until they were finished. One little baby named Teddy was set to have surgery later in the day. His brain was collecting too much fluid and the doctors were having to tap into his brain each week to drain it. Tapping in each which can become rather damaging so the doctors decided to send him to surgery to create a less harmful way of draining the brain fluid each week. After all the rounds were done and Teddy had gone off to surgery, each doctor sat down at their computers and uploaded information about each baby to their files. Dr. Te then went around examining each individual baby with a mini stethoscope. She had to change a few poopy diapers but was able to discharge a few of the babies to go home with their mothers. The doctors filled out more forms on their computer until lunch. At lunch I went with the med students to the cafeteria and talked with them more about the NICU and what they do. After lunch we reported to another c-section, but again didn’t need to take the baby to the NICU. This was one of the happier births where both mom and dad were excited. It was also interesting because the doctor that performs the c-section was the same surgeon who performed the hysterectomy at St. Charles that I watched. We went back and tended to babies that were fussy or needed to be examined. The med students spent the afternoon talking to Dr. Te about medical terminology and learning more about the NICU and infant health. One of the babies that I examined looked completely fine to me and I was wondering why the baby was admitted to the NICU. When I asked the doctors, they said the babies mom was a drug user and the baby had traces of cocaine, heroine, and other substances in her blood. Therefore, the baby was going to have to go through withdrawal before being discharged. The baby and all babies born in this situation are not considered addicted to drugs. They simply have drugs in their system. This can cause the baby an extreme amount of discomfort and irritability. To treat this, the doctors give the babies discomfort relieving medicine. The doctors slowly wean the babies off this medicine until they are recovered and no longer rely on drugs in their system. This is something I found extremely sad because after the baby is recovered the hospital legally has to hand the baby over to the parents who obviously in this case are drug addicts. I felt very bad for this baby because it will grow up in a rough environment and possibly pick up bad habits like her parents in the future.
0 Comments
After seeing a C-section when going to pick up a baby to transport it back to the NICU I wanted to know a more about it. Being that I witnessed a vaginal birth during week one, the implications of a C-section seem a bit more complicated.
A C-section stands for cesarean section and consisted of delivery a baby through an incision made in the abdomen and the uterus. C-sections are often planned ahead of time if the mom is experiencing difficulties, carrying multiple babies, or if she’s had a previous one. A C-section allows the doctors to quickly get the baby out without experiencing a possible traumatic vaginal birth. Some other reasons a mom may undergo a c-section is due to a stalled labor, if the baby is in distress, if there is a placenta problem, if the umbilical cord is in a knot, and much more. The first wheel the woman into the OR but a lot of times she has to be hooked up to an oxygen mask due to nerves. In terms of anesthesia, the doctors will usually use a regional anesthesia to allow the mom to be awake but feel nothing from below her chest. They place a catheter in the bladder to catch any pee and they put an IV in the arm to provide medication and fluid. The doctors wipe down the abdomen and use all sterile materials from the chest down. Each doctor must “scrub in” and remain sterile throughout the procedure. Keeping everything sterile is extremely important in procedures like this because the incision site could easily get infected if they don’t. The regional anesthesia allows the mother to be awake and hear/see everything is she wants to. Often times a curtain is placed between the women's head and abdomen to block her vision until the baby is out. To start the doctor makes an incision (usually horizontal but sometimes vertical) above the pubic bone. Once the doctor cuts through the fatty tissue enough to separate it, they will make a similar incision in the uterus. The doctor removed the baby, clamp the umbilical cord, and remove the placenta. While the baby gets cleaned, the doctor will close the incision with sutures. A c-section also requires recovery so they moms usually stay a few days at the hospital. For example, after we took the one woman's baby down to the NICU the doctors had to wheel her down about 5 hours later after she rested and recovered for a little while. Overall, the baby that came from the c-section we saw was taken to the NICU because of her breathing. The baby was having to work extremely hard to breath and when the doctors put her on oxygen she had to rely 60% on the oxygen because she was having a hard time. This is a common risk factor of c-sections. Because the baby was relatively good in size weighing around 5 lbs she most likely won’t have to stay in the NICU for a long time. In addition to this c-section, another set of doctors were in the other room tending to a vaginal birth where the baby's umbilical cord ripped off super close to the skin. They were struggling to get the clamp on and accidentally clamped the baby’s skin. Clamping the skin is bad because it can cause hard tissue to form there which leads to other problems. We prepared to bring up a portable incubator for that baby because the whole clamping situation was not looking good, but they tried again and were successfully able to clap just her belly button and stop any bleeding. I was surprised by how little the parents are down with their babies, majority of the time the NICU is very quiet. The babies are so tiny that when they cry, they hardly even make a noise. It’s much different that what you experience at an adult unit of the hospital. Because the patients are babies, the doctors simply examine them quietly and move on with their work. Finally, I am feeling better and was healthy enough to go to the NICU to shadow Dr. Te. After arriving at St. V’s hospital it took a while to navigate by way to the NICU. Once I got there and met Dr. Te, I was told to take off any rings or bracelets that I had on and to wash my hands. I then met a resident and med student and watched them fill out information about the patients on their computers. I used this time to ask questions about the NICU and about each patients case. Today the NICU had 15 patients ranging from a few minutes old to a few month old. Each baby had a specific condition or situation which was keeping them admitted to the NICU. One thing I found interesting from talking to the resident and med student was that they had a babies who was born at only 23 weeks. This is the youngest the child can be for the hospital to try to help them. Any younger and the baby would’ve been considered unhelpable. Dr. Te told me to follow the resident up to the Labor and Delivery unit where a C-section was scheduled to take place. I had to put on a full scrub gown, hairnet, boots, and facemask before entering the room. Unfortunately, the surgeon worked quick and the baby was out before we got there. The baby was taken to another room and examined. The resident and I watched the doctors monitor the baby and hook it up to oxygen. This baby was only 36 weeks and was having breathing difficulties. They decided it should be taken down to the NICU for further monitoring. We transferred the baby into a portable incubator and took it down. After being hooked up to a lot of monitors and machines the baby was left to rest. Majority of the day, the babies spend sleeping. When they aren’t sleeping, they are eating. Because the babies in the NICU can range in size they have to have equipment that fits every baby. Many of the smaller babies are fed through a feeding tube and the bigger babies are given a bottle. We then did rounds. Dr. Te, the resident, two med students, and a nurse went to each of the patients and read aloud what was going on with the patient and any changes that need to be made to their procedures. Everyone in the group took notes so that the NICU as a whole could all be on the same page. After rounds, we took a lunch break where I ate in the cafeteria with a med student. He talked to me a lot about the process of med school and residency. Then we went back to the NICU. The med student taught me how to “scrub in”, which consisted of using a pic and sponge to clean from all the way under the nails to the elbow. I put on gloves and then followed a nurse to an incubator to examine the baby. When I reached in the side holes of the incubator, the air inside was warm and moist. They made the humidity hirer for this baby so it’s skin could develop. The baby was about 2 pounds and had the tiniest little diaper on. He had been in the NICU for about a month and was born extremely premature. I used a mini stethoscope to listen to his heart beat. Babies heartbeats beat way faster than adults. The nurse taught me about the spots I’m suppose to look for on babies and other indication that the baby is doing well. After checking the baby, close the incubator and placed a blanket over it so he could sleep. After that, the resident and med students sat around Dr. Te for an information session. They asked her any questions they wanted, as well as, presented information about medical procedures to her. It was considered her teaching period. It was interesting to see how much knowledge she had about the NICU and how interested the med students were to learn. I will be going in to the NICU again tomorrow and doing roughly the same thing. I hope to get more hands on experience and hopefully get to see a C-section or other procedure. I planned to go into the office today at 9:30 am, however when I woke up, I had a fever, a headache, and a very sore throat. Unfortunately again, I was forced to stay home due to the potential risk that I could spread my illness to others.
Today I decided to research the pros and cons of giving birth at home verses giving birth in a hospital. A planned home birth is simply giving birth at home. It is necessary to have the assistance of someone who is qualified and experience with infant delivery; such as certified nurse midwife, a certified midwife, a midwife who has a license that meets international standards, or a doctor who practices obstetrics. There are pros to delivering a baby in your home. The pros can include delivering in a comfortable and familiar setting, controlling the delivery process, being allowed to deliver with religious and/or cultural expression, delivering without the pressure of using medications, and delivering with significantly reduced costs. In addition to the pros of delivering an infant in your home, there are also many significant cons to doing so. The most alarming con is that having an at home birth, increases the risk of infant mortality or serious injury by double-triple the amount of a hospital birth. Other cons include the possibility that your insurance will not cover the costs of at-home births, you might have to be transported to the hospital in case of an emergency, the dissatisfaction of hospital care, the need to create a birthing plan, the need to purchase medical supplies, and at-home births can be very messy. Is delivery at home right for you? This is a question that you must carefully consider and have meaningful conversations with your doctor or midwife. It is not advisable to have an at-home delivery if you have a high-risk pregnancy, if you are diabetic, if you have high blood pressure or preeclampsia, if you have experienced or at risk for pre-term labor, or if your partner is not in agreement with an at-home birth. Today I woke up ready to report to the NICU at 8 am; however, I was still feeling under the weather. I called Dr. Morelli and she told me that if I’m feeling sick at all there is no way the doctors at the NICU will let me in. Despite being healthy enough to go to school, the NICU is much different. I decided to research what an incubator is and what it does for the babies. An incubator is essentially an enclose crib the NICU babies are kept in that regulates their environments so they can thrive in their enclosed “habitat”. Each incubator can be set to different settings and temperatures to meet the need of each unique baby. The incubator can also protect the baby from outside allergens, light, and noise that are potentially harmful. Furthermore, the incubators can regulate humidity which helps develop the skin of the baby. As every baby is unique and have different needs, there are many different types of incubators. The first type is a close box incubator which filters the air minimizing the risk of infection. The sectioned type of incubator is called a double walled incubator can prevent moisture or heat from escaping. The third type of incubator is a servo-control which automatically adjust based on skin sensors attached to the baby. The fourth type of incubator is called an open box which regulates heat from below the baby but is open on all sides. The fifth type of incubator is portable which helps transport the babies to different wings of the hospital. I’m looking forward to going in tomorrow hopefully. My throat is still a little sore but everything else is feeling good. I’m actually kind of glad I got these two research days so I will be better prepared to observe on days to come in the NICU. So yesterday I got the flu which, unfortunately, kept me from going into the NICU. I have been puking a lot so I’m gonna do the best I can with this blog. I don’t know how much I will get done before I fall asleep again but we shall see.
I decided to do some research on the NICU and what it does. So to start off, the NICU stands for Neonatal Intensive Care Unit. This unit is essentially the ICU for ill or premature newborn babies. There a many reasons why newborns are admitted into the NICU; however, the first reason is for being premature. If a baby is born before completely 37 weeks inside the womb it is considered a premature baby. Premature babies often can’t keep their vital signs stable because they aren’t fully developed so they must spend time in an incubator to keep their vitals regulated. A second reason a baby may be admitted to the NICU is Respiratory Distress Syndrome. This syndrome is due to immature lungs. The NICU treats Respiratory Distress Syndrome by putting a oxygen mask or a breathing tube on the baby, depending on the severity of the case. A third reason a baby may be admitted to the NICU is infection. Newborns don't have the best immune systems and are more prone to get infections that they can’t fight off. This is the most common reason for neonatal death. This can be treated with antibiotics. A fourth reason a baby may be admitted to the NICU is Hypoglycemia. This is when the baby has low blood sugar. The low blood sugar is often a result of a mother who suffers from gestational diabetes. A fifth reason a baby may be admitted to the NICU is because of perinatal depression. This is when the baby has a traumatic birth or birthing complications which decreases the baby’s blood flow or oxygen flow. This is treated with a full body cooling treatment. While there are many more reasons a baby may go to the NICU these five seem to be the most common. I’m curious to see if this research holds true in my observations this week. Today was rather boring. I reported in a 9:00 am and followed Dr. Morelli on her morning rounds. I was amazed at how young the patients we saw were. Majority of the women we saw were 20 years old and pregnant.
When I seemed shocked by the fact that the patients were only a 1.5 years older than me, Dr. Morelli told me that she delivered a baby from a sixteen year old at 4am today. St. Charles is obviously not in the best area of town and as a result these patients, I’m assuming, aren’t wasting their money on contraceptives. When we walk into each patient's room it smells strongly of smoke. Unfortunately, these women are addicted to smoking and can’t stop during their pregnancy even when they know it harms the baby. Because around 85% of the women that come to see Dr. Morelli are smokers, I was curious of how much harm smoking actually causes for the baby. I found out that pregnant smokers tend to have their babies too early or give birth underweight babies. As a result, the babies are more likely to get sick and end up in the NICU. In addition, smoking prior to pregnancy makes it more difficult for women to get pregnant and if they do get pregnant they have a higher chance of having a miscarriage. Smoking while pregnant can also cause SID (sudden infant death). Dr. Morelli informed me that she sleeps at the hospital 14 nights a month because it is such a demanding job. People come in to give babies all the time and it takes many hours so Dr. Morelli has to be ready at all times to deliver those who need her in the early hours of the morning. In addition, she not only has to present during the deliveries but she has to assure the patient that they are in good hands and be happy and cheery even when she’s exhausted. On Monday I will be watching another hysterectomy without a robot done by Dr. Greenbaum. I’m curious to see how different the procedures with and without a robot are. After the procedure I will then go to the NICU and get to see babies. Today I had yet another crazy day. I arrived at 9:30 in Dr. Morelli’s office, where gave me scrubs to change into. We walked to the hospital and she got me a surgical jacket and passed me off to a med student who took me to the operating section of the hospital. She took me to meet the patient in which I’d observe. The patient was extremely nervous and was being put on medication to calm her down. She was getting a hysterectomy which removes her uterus and her fallopian tubes from her body. The reason she was getting this procedure done was because she had endometriosis which causes her pelvic pain. Endometriosis is when the tissue that normally lines the uterus grows outside of the uterus and can cause pain. After that, we found the room I was supposed to observe in and waited outside.
While we were waiting for the med student taught me how to “scrub in”, which basically consisted of thoroughly scrubbing every millimeter of your hands and forearms. I then put on shoe covers, a hairnet, and a face mask. When I got into the OR the patient had just been sedated and as a result, pooped all over. The nurses had to clean everything up and then “re-scrub in”. It was extremely interesting to see how sterile they had to keep everything in the room. Everything that was used came out of a sterilized package. I was afraid to touch literally anything because I didn’t want to desterilize anything. This hysterectomy was especially cool because it was a laparoscopy-assisted robotical. This means that four small incisions were made into the patient's stomach. A camera was inserted in her belly button, robotic arms were inserted in two of the holes, and a tube that pumped her full of gas was inserted in the remaining hole. In addition to all that, there was a rod and cup inserted into her vagina which allowed the med student to move and manipulate the uterus while the surgeon worked to cut around it. The surgeon then moved over to machine in the corner of the room which controlled the robot arms and he began the surgery. He burned the fallopian tubes off and had a nurse pull them out through one of the incisions. Then he began to burn around the uterus which I got to watch from a screen since it was all done with robot arms and cameras. After a little while, the surgeon offered the resident to come work the robot. The resident was much slower at working the robot but the surgeon talked him through it. Later the surgeon hopped back on the machine finished up the procedure. The med student then pulled the detached uterus through the vagina. It was extremely small because the woman has never had a baby. The surgeon then had to stitch up the spot where the uterus used to be and spray cooling stuff on the burns inside the patient. When the surgery was all said and done the doctor had to check to make sure they didn’t puncture the bladder. They tested this by pumping the bladder with water and watching to see if pee would come out of the ureters. It took a long time, but eventually, pee did come out and they were able to call the surgery a success. They pulled out all of the tools in her incisions and deflated her stomach. The med student and resident then proceeded to stitch up her incisions. When I asked about the recovery time, the doctors said that this patient would be walking by tonight because the recovery process is very quick for laparoscopy procedures. Because they only have to make small incisions, those four little stitched up area on her stomach will be the only thing that’s sore for her tonight. While I’m extremely afraid of needles and blood, I can confidently say that I conquered my fear tonight. It was so impressive to see the precision the robot had and how everyone in the OR worked together to perform this procedure. I thought I was in the OR for 45 minutes but when I left I realized the procedure had taken three and a half hours. I guess time flies when you’re having fun. Yesterday during my rounds at St. Charles hospital I got to see the sad part of being an OB-GYN. A 27 year old patient came in concerned about her inability conceive a baby despite trying with her husband for over a year and a half. Her husband took a semen test and everything looked fine so it seemed to be her body that was not allowing her to get pregnant. There were a lot of medications Dr. Morelli suggested that they put her on but I didn’t know enough about infertility to understand much of what was going on. So today I decided to research it due to no doctors being at the hospital to shadow.
The definition of infertility is basically any couple who fails to conceive a baby after a year of unprotected intercourse. There are different types of infertility as well. It’s often broken up into disability, primary, and secondary infertility. Disability infertility is extremely common in women in developing countries. It most often due to unsafe abortions or a bacteria in the womb. This is classified as a disability because it is an impairment of a function. The second type of infertility is primary infertility. This when a woman can’t get pregnant or spontaneously miscarries a baby. The third type of infertility is when a woman can’t get pregnant and/or spontaneously miscarries a baby multiple times. Infertility can become extremely frustrating because there are so many different reasons it can happen. It can be something wrong with the male's sperm being low in count, slow, weak, or abnormal due to hormonal imbalance, testicular cancer, overheated testicles, and much more. It can also be something wrong with the woman body such as age, smoking, alcohol, obesity, STI’s, mental health, ovulation disorders, problems in the fallopian tubes, and much more. Because there are so many factors that go into fertility and so many possible things that could go wrong, it takes a lot of tests for both the males and females to figure out what the problem is. In addition, there is no one cure. There are many different treatments but not all are successful. There are a lot of different oral medicines, injectable drugs, fallopian tube surgical procedures, sperm injection, and more that can treat someone with infertility. Yesterday, Dr. Morelli prescribed the infertile woman Metformin, an oral drug, with the hope that she becomes fertile. In addition, the woman was instructed to follow a very specific intercourse schedule to give them the best chance of conceiving a baby. Today was a lot more exciting. I showed up at 8:45 at the office and from their Dr. Morelli (Mrs. Greenbaum) walked me to the Labor and Delivery unit at the hospital. I changed into scrubs and watched a day old baby get circumcised. To be honest, it broke my heart a little to watch because it looked so painful. She began by injecting the baby with medicine, prying open the urethra hole, and inserting a metal rod. She then made a slit in the skin and peeled it back from the rod. She cut the access skin off and that was it. The procedure took around 2 minutes but the baby screamed his head off during the whole thing. The nurse put numbing medicine on the baby and wrapped it in a diaper.
After the circumcision was finished we checked up on a woman in labor. This woman was scheduled to go to prison today but instead, she was delivering her baby. She even had an ankle bracelet on. She was six centimeters dilated and had to wait on her boyfriend to wake up so she could ask him if she was “allowed” to get an epidural. Because labor can be a very long process, Dr. Morelli and I walked back to the office to do some rounds before the woman gave birth. I learned that Dr. Morelli deals with more of the pregnant women, whereas, Dr. Greenbaum does more of the problem checkups. Dr. Morelli used a doppler monitor to check on the patients’ bellies which amplified the babies heartbeat. We got through about two checkups when we got a frantic call from the hospital saying the women we checked on before was pushing and the baby was coming quick. Dr. Morelli and I sprinted as fast as we could back to the hospital where we made it just in time. The woman had just gotten the epidural only five minuted before and it hadn’t kicked in yet. She was in a lot of pain and was yelling. She pushed super hard twice and out popped the baby. There was a lot of blood and a lot of gross bodily fluid flying everywhere that I skillfully dodged it. They immediately laid the baby on the mother's chest so that it would be skin to skin. While the baby is in the womb it gets glucose from the placenta, so when it’s is born and separated from the placenta, they put the baby skin to skin with the mother to help regular the babies blood sugar levels. The blood sugar levels give the baby energy. The woman had a very full bladder which had to be drained causing a painful burning sensation that she was not a fan of. This was her 10th child... crazy. In addition to that, Dr. Morelli had to get the placenta out which was a painful process because the epidural still hadn’t kicked in. While it was all exciting, Dr. Morelli’s job was done and it was left to the nurses and residents to do the rest. We left and went back to the office. We saw close to 30 patients. The patients were mostly pregnant women getting their check-ups or women wanting tubal ligations. This procedure is medical sterilization to prevents women from having any future pregnancies. I watched one biopsy similar to the one I saw yesterday; however, Dr. Morelli couldn’t get the patient's cervix to open so she had to send her to the hospital to get the procedure done. Overall, it was a very eventful day and I’m excited to be in the labor and delivery unit all day tomorrow. |
WITHDRAWALC-Section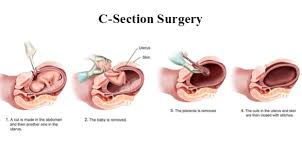
C-Section curtain
Incision location
Baby size during pregnancy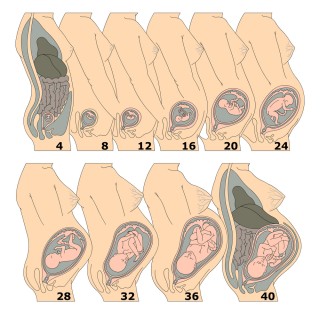
PReemie Diapers
NICu
laparoscopy-assisted robotical
Endometriosis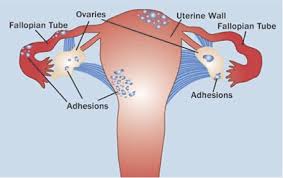
laparoscopy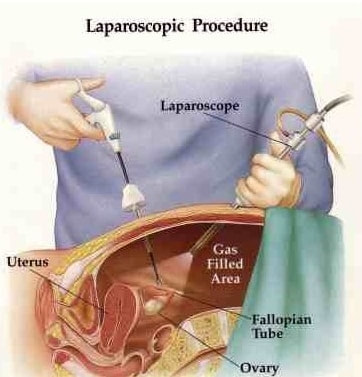
Doppler monitor
Circumcision Tools
Tubal Ligation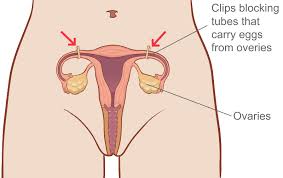
Speculum
Fibroids
Ureteroscope
|
